Archive for the “Microbiology stories” Category
Recently, I have been working on an essay for my last year in college. I titled it: “Parkinsonism: Disease and Treatment”, scary enough? NO!!?? I turned it in, anyway. In it, I identified the neurodegenerative disease that targets the basal ganglia and deprives it of the inhibitory neurotransmitter (NT), dopamine. No dopamine means no balance between the excitatory action of the NT, Acetylcholine, and the inhibitory action of dopamine, leading to the well-known clinical picture of parkinsonism that Jankovic (2007) gave the acronym TRAP: Tremor at rest, Rigidity, Akinesia/bradykinesia and Postural instability.
Parkinsonism can be classified into:
- Primary/idiopathic “of unknown cause” which is mostly due to degeneration of dopaminergic neurons (a.k.a Parkinson’s disease)
- Secondary to viral infection as encephalitis & meningitis; drug-induced, e.g., antipsychotics; or due to brain damage caused by trauma, anesthetics, or toxins as MPTP (a contaminant of street-drugs).
 Arvid Carlsson You may know that the Nobel Prize associated with Parkinson’s disease didn’t go to Dr. James Parkinson who described it in an essay he wrote back in 1817 calling it “The Shaking Palsy”. It went jointly to Arvid Carlsson, Paul Greengard, and Eric R. Kandel in 2000 (To find out more about the story, here’s the Nobel lecture by Dr. Carlsson). Carlsson and colleagues discovered dopamine as a potential NT in 1957. After that, in 1960, Hornykiewicz and his postdoctoral fellow, then, Ehringer observed the decrease of dopamine levels in Parkinson’s disease patients, and levodopa successful trials started after that, in 1961.
 J. Robin Warren What does Dr. Warren, the scientist whose discoveries led to a paradigm shift in physiology, who said out loud that peptic ulcer is an infectious disease caused by Helicobacter pylori, the gut bacteria? What does he have to do with parkinsonism? Note that: J. Robin Warren and Barry J. Marshall also won Nobel prize in medicine for 2005 for their discovery.
Helicobacter-induced parkinsonism!!
What I am trying to say here—and didn’t say in my essay—is that there is a hypothesis, Helicobacter-hypothesis, that strongly provides another cause of idiopathic parkinsonism, which will not be idiopathic any more, and this cause is H. pylori (Altschuler, 1996). Or to be more accurate, I will say parkinsonism associated with H. pylori. Dobbs and colleagues have carried out well-controlled studies and observed a significant conversion in patients with Parkinson’s disease from malignant into benign parkinsonism after successful eradication of their H. pylori, even with no levodopa administration. The rationale behind this theory is that: H. pylori induces an autoimmune reaction against mitochondria, then a systemic inflammatory response with the whole gang of inflammatory mediators and antibodies reaching and crossing the deficient areas or areas with increased permeability of the blood-brain barrier, causing parkinsonism. And the blood profile can prove the Helicobacter-hypothesis.
Tags: Arvid Carlsson, blood profile, essay, Helicobacter pylori, Helicobacter-hypothesis, idiopathic, J. Robin Warren, James Parkinson, levodopa, Nobel Prize, Parkinson's disease, parkinsonism, shaking palsy, systemic inflammatory response, TRAP
 No Comments »
No Comments »
“Get me more, mummy!” demands one youngster bacterium, pointing to the drops of antibiotic reaching the colony headquarters.
Come on! FOR REAL?
Sadly very true and it is not even that infrequent either! I only became aware of this after reading about a study, where researchers in HMS, led by Dr. George M. Church, collected soil samples in an experiment, attempting to search for more bio-diversity and were stunned to see that as they added antibiotics to these bacterial cultures, the bacteria didn’t seem to mind at all!
Unlike human beings, bacteria tend to like sharing. The more they share their strategic defenses, the more prosperity they end up living in. Again, to our dismay, such fear was translated into reality, as t his has already extended to the pathogenic minorities of the bacterial world in a new study, published in January in the International Journal of Tuberculosis and Lung Disease. Scientists, in China, have stumbled upon a strain of tuberculosis-causing bacteria, called Mycobacterium tuberculosis, INCAPABLE of growing adequately in the absence of rifampicin. This is as ominous as such news can get. his has already extended to the pathogenic minorities of the bacterial world in a new study, published in January in the International Journal of Tuberculosis and Lung Disease. Scientists, in China, have stumbled upon a strain of tuberculosis-causing bacteria, called Mycobacterium tuberculosis, INCAPABLE of growing adequately in the absence of rifampicin. This is as ominous as such news can get.
This strain was discovered as physicians attempted to treat a TB-infected patient with a regimen which included rifampicin. Unexpectedly, his condition worsened and only upon the removal of rifampicin did he start feeling better, until eventually full recovery. Already, reports of multidrug-resistant TB “MDR” have been around for some time. Normally, the treatment course includes more than 1 drug to be able to effectively kill the bacteria. Apparently, the bacteria have found a way to get around that!
We can only wonder: which antibiotic is next?
Tags: antibiotic, antibiotic resistance, bacteria, harvard, tuberculosis
1 Comment »
Is it a luxury to “think like a microbe” and to publish blogs such as “Adopt a Microbe“ and books like “The Other End of the Microscope: the Bacteria Tell Their Own Story“ (find it on Google Books)? Is it just about understanding or “getting to know” bacteria, or is it a necessity to be “microbe-oriented” for better understanding of pathogenesis and for developing the appropriate eradication and prevention strategies (I can’t think of better examples other than Reverse Vaccinology and H. pylori)?
When I first read this commentary “The Case for Biocentric Microbiology”* by Dr. Ramy Aziz, published by the journal “Gut Pathogens, I was shocked! The article was presenting a very different perspective, at least different from what I always dreamed of as a pharmacy student, to kill the bad bugs by designing an effective, highly selective chemotherapeutic! Plus it was my first time to read an opinion article, and I used to take the microbiology courses for granted; “this is a bad microorganism, causing this bad infectious disease with serious manifestations including these, diagnosed by the following and the antibiotic of choice is this.” And then Dr. Aziz came with this article with the cool, simple and exciting writing style that keeps one alerted the entire article, gathering all those thoughts and examples of our human-centered/self-centered view of microbiology.
Four parts I enjoyed the most in the commentary:
- The tabular form of “differences between the anthropocentric and biocentric views of microbes.”
- The final balancing paragraph –the conclusion.
- The “competing interests” part, which is funny.
- The questions part, which is an excellent idea to open up discussions, especially for those who are not-natural-born brain stormers like me!
Even though microbiology is a new science, it suffers from anthropocentric view that Galileo suffered from; starting with the field’s name itself, “microbiology” -liked what Dr. Elio Schaechter mentioned: “Small,” says who? Not the microbes… till the funding agencies that give priority to studying bad microbes (i.e., pathogens), and good microbes (i.e., fuel-producing and yogurt-making bacteria) nothing else!
 Bacteria convention - http://www.towardslife.com/ We, in our human-centered view; automatically classify any newly-discovered bacterium to fall into one of three categories: the good, the bad and the ugly… no, not that one! They are: the useful guys, the harmful guys and the just-existing guys. Now, let’s take a look at the biocentric view of microbes: Humans and microbes share many ecosystems. To microbes, humans are just an ecosystem that is a “relatively safe” habitat with a source of nutrition.
As victims, we think about pathogenesis/infection as it’s shedding from the immune system, invasion and toxin production; but microbe-oriented microbiologists/bacteria whisperers know that, to bacteria, pathogenesis is just defense, seeking nutrition, and excretion of metabolic byproducts. Being pathogenic or opportunistic is not their reason of existence, it’s just a form of adaptation to survive in this hostile environment (aka the human body).
You do not believe me!? OK, bacteria lived –happily- thousands of millennia before mammals and humans, so their reason of existence can’t be to harm humans, like what Dr. Aziz is mentioning: “Who attacks whom”, are the bacteria the “one” that start the fight, or is it the human immune system that starts the war against them? A very interesting example to understand adaptation is Legionella pathogenesis, and how they adapted to human macrophages because they used to survive in amebas, which are similar to our macrophages.
Back to the basic question, is it a luxury or a necessity?
Studying “all” bacteria from their perspective will help us in understanding pathogenesis and subsequently developing strategies to combat infectious diseases (immunization and design highly selective chemotherapeutics), will give us a better idea of the tree of life and the metabolic map, and studying environmental microbiology will allow us to meet new “useful” microbes like what happened with the PCR Taq-polymerase, we knew how to make use of this bacterial polymerase that can work at those very high temperatures required for the PCR steps.
Here are two interviews about the commentary covering two segments of readers, the first one is with Dr. Betsey Dyer, Professor of Biology at Wheaton College, and the second one is made with Radwa Raed, a micro-writer and a final-year FOPCU student:
1- What is your opinion about (the commentary)? To what extent do you find it compatible with your bacteriocentric view of bacteriology? How strong are the arguments?
Dr. Betsey D. Dyer, Professor of Biology at Wheaton College.
“I thoroughly enjoyed Ramy Karam Aziz’s article “The Case for Biocentric Microbiology.” I think he is absolutely right that some old fashion thinking about the divisions of microbiology and anthropocentrism in general have hindered a more complete understanding of the microbial world. I also think Dr Aziz is quite bold and daring. I’m not sure I could have gotten such forceful statements accepted for publication! Good for “Gut Pathogens” to print it! I hope Dr Aziz gets lots of readers and citations.”
2- How did (the commentary) change your point of view? Are you with or against the biocentric view for microbiology? Do you think about it as a view against, or at least far from, your beliefs as a pharmacy student dreaming of fighting diseases? What are your opinions regarding studying environmental microbiology in pharmacy school?
Radwa Raed, Pharmacy student, Faculty of Pharmacy, Cairo University – Egypt.
“From my humble point of view, I would have to agree (with the biocentric view of microbiology). It goes without saying that studying more about certain bacteria “the ones some would consider to be of the least priority” will definitely expand our knowledge about the overall, and in many cases analogous or even similar, methods of survival, adaptation to existing conditions, etc.., which all pretty much ultimately serve medical microbiology. Plus, leaving a whole chunk, simply unexplored, can only raise several “what if” questions; one of which, that comes to mind, is what if the simplicity and less dramatic forms of life could help researchers better grasp the machinery behind these fascinating little creatures 🙂
As for studying environmental microbiology in pharmacy schools, I would have to oppose the idea, because the field of pharmaceutical science is taught so the future students can come to understand, and hopefully later suggest, treatment methods against pathogenic microorganisms, prophylaxis, and so forth..so studying the harmless ones would not point in this direction. It can only lead them to drift away from the pharmaceutical science branch of study into a more microbiology-oriented career.”
You can read the paper, share your comments and debate the arguments here, and you can also vote for it on BioWizard.
––
*Full Citation:
Aziz, R. (2009). The case for biocentric microbiology Gut Pathogens, 1 (1) DOI: 10.1186/1757-4749-1-16
Tags: adopt a microbe, anthropocentric, bacteriocentric, Betsey D. Dyer, biocentric microbiology, commentary, competing interests, environmental microbiology, gut pathogens, H. pylori, metabolic map, microbe-oriented, microbiology, pathogenesis, pathogens, PCR, Ramy K. Aziz, reverse vaccinology, taq-polymerase, the case for biocentric microbiology, the other end of the microscope, tree of life
No Comments »
Did you see some one before who can fly without wings or move without legs? You will answer : definitely no, but I know someone, or better yet some living thing, who can do just both and it is called Borrelia burgdorferi; let’s share its story. It is a loosely coiled bacterium belonging to a class called spirochetes (moving bacteria).
 Borrelia burgdorferi Borrelia burgdorferi is motile through the undulation of its axial filaments. It is transmitted to humans by the bite of infected ticks (Ixodes scapularis and Ixodes pacificus) and cause a serious progressive disease called lyme disease.
The story of lyme disease began in 1975 when a mother, with her children in lyme city in the United States, was admitted to a hospital with signs of rheumatoid arthritis. It was a mysterious case until the discovery of Borrelia burgdorferi and that is how the disease got its name, when it was discovered in 1982. Symptoms and signs of lyme disease can be categorized into three phases:
Phase (1): An early localized skin rash, characterized by inflamed red edges with a clear white center at the site of insect bite, appears and is called “erythema migrans“.
 Erythema migrans Phase (2): The rash resolves as the bacteria begin to move into the blood stream towards their target organs like large joints, heart, and nervous system.
Phase (3): Inflammation of heart muscle leads to abnormal rhythm, meningitis, confusion and finally arthritis.
Treatment in the early phase is an easy mission by amoxicillin or doxycycline, orally for few weeks. However, the recommended regimen in late stages include parenteral ceftriaxone, analgesics to control the severe pain, and anti-inflammatory drugs, usually required for months .
Images credits:
Borrelia burgdorferi: http://www.wadsworth.org/databank/hirez/hechemy2.gif
Erythema migrans: http://phil.cdc.gov/PHIL_Images/9875/9875_lores.jpg
Tags: bacteria, Borrelia burgdorferi, erythema migrans, lyme disease, meningitis, outbreak, rheumatoid arthritis, ticks (Ixodes scapularis and Ixodes pacificus)
2 Comments »
Seriously, these days, no matter where I turn to, there is somebody contracting some form of bacterial infection that turns out to be pretty serious. At the beginning of the new year, a 20-year-old perfectly fit Brazilian model died of what appeared to be a Pseudomonas aeruginosa infection. As far as I know, polymyxins should work like a charm. Sadly, her life ended after enduring the amputation of her limbs and a nephroectomy procedure in an attempt to save her. And now again, rumor has it that Michael Jackson contracted a MRSA infection following a nose job.
Where did the antibiotics go? Is the bacterial resistance way ahead of us that we can’t even keep up? In a field study conducted amongst fellow neighbors & relatives, many did infact admit that they go rushing to their local pharmacies demanding a prescription of antibiotics for a mild flu or a fever of 38 degrees. Not that that is worse enough, they don’t comply to the pharmacist’s orders “if he did infact give an order” to administer it for the full course of the medication.
This should be a warning sign…an alarm triggering off right about now. Developed countries are already facing these problems, we shouldn’t be lingering around. Public awareness campaigns, maybe similar to those concerning the bird flu being aired these days, ought to be held. Our community is in desperate need of our expertise to guide, inform, and advise them about the consequences and potential threats at stake here.
“The window is closing and we’re coming to the end of the antibiotic era,” said J. Glenn Morris Jr., M.D., who heads the division of hospital epidemiology at the University of Maryland School of Medicine, College Park, MD. This was in 1999.
Can we really beat antibiotic resistance? or are bacteria getting the best of us?
Tags: bacterial resistance, brazilian model, c8bcf5c0dc8cfaa24f17995e7625c2b0, michael jackson, MRSA, pseudomonas
1 Comment »
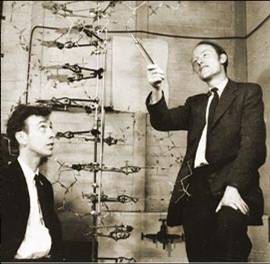 On February 28, 1953, James Watson and Francis Crick announced to their friends that they have discovered the chemical structure of the DNA. After publishing their paper in Nature on April 2, the official announcement took place on April 25. On February 28, 1953, James Watson and Francis Crick announced to their friends that they have discovered the chemical structure of the DNA. After publishing their paper in Nature on April 2, the official announcement took place on April 25.
That is what I have read in Al-Ahram newspaper today. What a discovery! Imagine if they had not done it, we would have had no clue about genes & protein synthesis, no recombinant DNA tech- & no sequencing. We would have had no molecular biology departments in universities! Abby from NCIS & Greg from CSI would have had no job!
So, what was the real story? To what extent are the “rumors” saying that Rosalind Franklin is the real discoverer of the DNA double helix right? Is she really the “Dark Lady of DNA”?
I hope we can get the story through your comments after we read this:
1- Crick papers from the National Library of Medicine.
2- Watson’s interview with a group of top North Carolina high school students in 2003.
3- BBC celebrating the 50th anniversary of DNA structure discovery in 2003. (really interesting)
4- Rosalind Franklin: Dark Lady of DNA by NPR (National Public Radio)
Image credits:
Watson – Crick DNA model: http://www.cs.princeton.edu/
Rosalind Franklin: http://www.npr.org/
Tags: 1408f278d2a6f884de58c0c44b7a6af7, DNA, Francis Crick, James Watson, Rosalind Franklin
No Comments »
 If you try to search in the library or over the internet for AIDS, you will find a huge amount of information available. You will also figure out that all scientists reach a dead end at the step of treating or vaccinating against AIDS. Their stop makes you never stop thinking: why can’t they continue? Why is there no cure for such a disease? Or at least why can’t they stop the progress of this illness by simply making a vaccine? It is like reading the same book millions of times without understanding its end, then you re-read the last chapters but still “YOU CAN’T”!! If you try to search in the library or over the internet for AIDS, you will find a huge amount of information available. You will also figure out that all scientists reach a dead end at the step of treating or vaccinating against AIDS. Their stop makes you never stop thinking: why can’t they continue? Why is there no cure for such a disease? Or at least why can’t they stop the progress of this illness by simply making a vaccine? It is like reading the same book millions of times without understanding its end, then you re-read the last chapters but still “YOU CAN’T”!!
I think that we need to restart reading the book from its beginning. We need to re-read about the origin of AIDS infections, to know more about HIV genome, and how its genes function; then we may know how to slow down or terminate progression of the virus inside the human body or at least to stop its passage from an individual to another. Hence, we may be able to read the book again and this time we can understand its end.
AIDS was initially reported on June 5th, 1981. But, it is more precise to mention the first documented AIDS case, which was in 1959. At that time, no one was able to define such an illness; however, scientists did a favor for the humankind by preserving the infected tissues till someone would be able to define HIV, i.e. after 1981. I may ask why not before 1959? But who can answer a question like this?
The origin of AIDS has so many controversial theories, including conspiracy theories. One of these is that HIV arose as a result of leakage in the US governmental or military labs during the development of a biological weapon. You may ask Dr. Leonard G. Horowitz (the author of Emerging Viruses: AIDS & Ebola. Nature, Accident or Intentional? And Death in the Air: Globalism, Terrorism and Toxic Warfare) for evidence to prove such an idea. As wikipedia page of ” AIDS origins opposed to scientific consensus” mentions his theory which claims that AIDS virus was engineered by such U.S. Government defense contractors as Litton industries for the purposes of bio-warfare and “population control”.
Dr. Alan Cantwell (the author of AIDS and the Doctors of Death) supported this theory, by naming one scientist that led the US military research on homosexual and bisexual men between 1979 and 1981; he attributed these research activities to Dr. Wolf Szmuness. And, when Dr. Alan was asked about the cases that were reported before 1979, his answer was that the American media masked the truth at that time! This has been also mentioned on “AIDS origins opposed to scientific consensus” Wikipedia webpage.
Another unreliable hypothesis had been advanced by Edward Hooper, as he accused Hilary Koprowski, the polish virologist and immunologist who was preparing polio vaccine using tissue cultures from non-human primates during 1950s, that he might have transferred AIDS from monkeys to human. This idea couldn’t be evidenced when one of these vaccine vials had been checked in 2000 to show negative HIV or SIV (Simian immune-deficiency virus that infects chimpanzees). Also, by checking the protocols of that old research, it is clear they were working on monkeys’ kidney cells that cannot transmit AIDS. But can one negative vial become a prove for the whole negativity?!
The most accepted and recent theory assumes that HIV is an evolution from SIV. This Cameroon Chimpanzees theory was suggested in 2006 after a study on genetic samples from more than 1300 chimpanzees within 7 years by Dr. Beatrice Hahn. It seems that one person had been bitten by one of these apes or got cut while he or she was trying to slaughter one of these animals, maybe for eating purposes!!
If this Chimpanzee in the picture is the main suspect now for HIV triggering on earth, the question now is: Do we have current reports for the same transmission from apes to human? If yes or no, I think we need to re-study and search that SIV which might tell us something about its “daughter” HIV (as accepted by most of the scientists). It is like reading the book from its beginning not the last chapters, sure it will tell us new things.. Like what? I really dont know, it may be like the first idea that led to inventing the nuclear bomb, would you believe me if I told you more than 60 years ago that there is an idea to bombard the nucleus to make a huge bomb? It was just an idea, but the know how was not known. I think it is the same for the AIDS book: we need to re-read but we still don’t know what is going to happen after that reading. All I know that we need to re-read with a new vision, not the same ordinary way of reading.
Image credits: http://upload.wikimedia.org/wikipedia/commons/8/8d/South_Djoum_Chimp.jpg
Tags: AIDS, AIDS origin, Cameroon Chimpanzees hypothesis, Consiperasy Theories, conspiracy theories, Dr. Alan Cantwell, Dr. Beatrice Hahn, Dr. Leonard G. Horowitz, Dr. Wolf Szmuness, Edward Hooper, Hilary Koprowski, HIV, SIV
7 Comments »
Hello, hello. You’re now tuned to your favorite blog: micro-writers.egybio.net. Tonight we have this very special guest, live, online. After two months of waiting, we finally got this exclusive interview with the emerged Streptococcus pyogenes strain, the most dangerous ever, M1T1. We have it here, with us, in the studio.
– Hello, M1T1. Welcome in our studio.
– Hey there.
– We knew from our resources, which are totally classified, that you got yourself in trouble recently.
– (Interrupting), I did NOT get myself in trouble. EID set me up.
– M1T1, Would you please calm down & tell us a little more about yourself?
– Well, I belong to Group A streptococci (GAS) aka Streptococcus pyogenes. M1T1 is my serotype; I’m just a clonal strain. As you know, S. pyogenes colonize human skin & throat causing either non-invasive (sore throat, tonsillitis & impetigo) or invasive (necrotizing fasciitis NF, scarlet fever & streptococcal toxic-shock syndrome STSS) infections. Actually, NF gave me my nick: Flesh-eating bacteria.
– So, you cause all people NF & STSS?
– No, kid. It depends on their genetic susceptibility, what you call “Host–pathogen interactions”. I was isolated from patients with invasive as well as non-invasive infections during 1992–2002. This is NOT entirely my fault; humans can make me extra virulent by selecting the most virulent members.
– Back to your history, when have you exactly been isolated?
– M1 & her sisters were the worst nightmare in US & UK in the 19th century as they caused the famous pandemic of scarlet fever. “Nevertheless”, early 1980s was the golden age of my strain as well as my very close sisters M3T3 & M18. We caused STSS & NF in different parts of the world. Great times, great times!
– Only for you, I suppose! So, what made you hypervirulent? What caused you this “epidemiologic shift”?
– Two reasons Dr Ramy K. Aziz identified that improved my fitness to humans: the new genes I got from phages & “host-imposed pressure”. Both resulted in the selection & survival of me M1T1 the hypervirulent strain. Dr Aziz’s work at Dr Kotb’s lab resulted in identification of a group of genes I got from phages that changed my entire life.
– Interesting! Tell us more about that. How did phages “change your life”?
– Dr Aziz proved that I differ from my ancestral M1 when he found that I have 2 extra prophages (lysogenized phages didn’t get the chance to lyse me, so they became integrated in my genome):
1. SPhinX which carries a gene encodes the potent superantigen SpeA or pyrogenic exotoxin A (scarlet fever toxin).
2. PhiRamid which carries another gene encodes the most potent streptococcal nuclease ever, Sda1.
3. He also found that phages conversion from the lytic state to the lysogenic state resulted in exchange of toxins between our different strains (aka Horizontal Gene Transfer). Phages are very good genetic material transporters, what makes “strains belonging to the same serotype may have different virulence components carried by the same or highly similar phages & those belonging to different serotypes may have identical phage-encoded toxins.” What a quote from Rise and Persistence of Global M1T1 Clone of Streptococcus pyogenes.
– Well, It was not that interesting. So, what? What’s the significance? How that made you hypervirulent?
– You can’t get it? You’re not that smart, are you? Tell me, what made M1 hypervirulent causing scarlet fever in the 1920s and me hypervirulent causing STSS in the 1980s with a 50-years decline period?
– Superantigen?
– Exactly. You do have your moments! Superantigen encoding-gene was present in us and absent in strains isolated in the period between them. The interesting part, for me of course, that humans after 50 years of absence of hypervirulent strains had absolutely no superantigen-neutralizing antibodies. That was the real invasive party. Superantigen causes high inflammatory response because of its non-specific binding to immune system components (antibodies & complements) causing an extremely high inflammatory response. In fact, SuperAg inflammatory response is “host-controlled”.
– So, what about Sda1?
– Streptodornase (streptococcal extracellular nuclease) helps me to degrade neutrophils that entrap me in the neutrophil extracellular traps (NETs). So, I can invade humans freely & efficiently and be able to live in their neutrophils. Dr Aziz proved in his paper “Post-proteomic identification of a novel phage-encoded streptodornase, Sda1, in invasive M1T1 Streptococcus pyogenes” that it’s all about C-terminus in my Sda1; the frame-shift mutation increased my virulence while deletion decreased it.
– Now we know about your SuperAg & nuclease (DNase), what’s the “host-imposed pressure”?
– I have my own SpeB (Protease), I use it to degrade my other proteins (virulence factors), which provides me with a good camouflage & gives me access to blood. When the host immune system recognizes me, it traps me in NETs. At this time, I secret Sda1 to degrade neutrophils. Actually, SpeB protects you, humans, from my Sda1& my other toxins. When SpeB was compared in patients with severe & non-severe strep infections, it was found that SpeB wasn’t expressed in case of severe infection. Expression of SpeB may be host-controlled, as host selects the mutants with a mutation in covS, a part of my regulatory system which regulates my gene expression including SpeB gene.
– Finally, M1T1. How do you see your future?
– More new phage-encoded genes, more selection of the hypervirulent strains by the host & more regulation of expression of my virulence factors. Pretty good future! I also count on humans to not develop immunity against me like what happened in 1980, when I got new virulence factors or allelic variations in my old ones.
Thank you, M1T1. Pleasure talking to you…….M1T1? M1T1, where are you? Why do I feel this strange pain in my throat?
Image credits:
Streptococcus pyogenes: http://adoptamicrobe.blogspot.com/
Tags: covS, epidemiologic shift, flesh-eating bacteria, global M1T1 clone, group A streptococci (GAS), horizontal gene transfer, host-imposed pressure, host–pathogen interactions, impetigo, M1T1, Malak Kotb, necrotizing fasciitis, neutrophil extracellular traps (NETs), phage-encoded toxins, pyrogenic exotoxin A, Ramy K. Aziz, S. pyogenes, scarlet fever, sore throat, streptococcal nuclease Sda1, streptodornase, STSS, superantigen SpeA, tonsillitis
5 Comments »
It’s hard to talk about someone you know who passed away, but, believe me; it’s harder when you talk about someone you know nothing about. To know someone better, you have to read his writings or, simply, read what his friends wrote about him. Reading what a disciple of his, David M. Morens the director of the National Institute of Allergy and Infectious Diseases, wrote about him made me believe that Dr. Gregg is the luckiest person on the planet by gaining this undeniable love & appreciation from his students. Dr. Gregg died on July 9, 2008 at the age 78.
Michael B. Gregg, M.D. was born in 1930 in Paris, France. He was educated at Stanford University and Western Reserve University School of Medicine. He entered the Public Health Service in 1959 right after he completed his residency in internal medicine at Columbia Presbyterian Hospital in NY. He first served at the National Institutes of Health Rocky Mountain Laboratory. He then trained in infectious diseases in Lahore, Pakistan before he joined CDC (it was known as the Communicable Disease Center) in 1966 as Chief Epidemic Intelligence Service Officer (EISO). From 1967-1988, Dr. Gregg (or Mike like everyone in the CDC used to call him) was the editor of the MMWR. His writing style “just the facts” made thousands of epidemiologists believe that good medical writing indicates clear thinking, which is the only thing needed in Epidemiology. In 1975, Mike was the MMWR editor, Viral Diseases Division director and deputy director of the Bureau of Epidemiology.
Mike was not only a MMWR editor, but he taught hundreds of students in NIH & CDC to become leaders in epidemiology & public health. Mike’s textbook “Field Epidemiology” (Don’t get extremely excited, It’s a link to the review not the book itself. My apologies.) is the “go to” book in breakout investigation & to solve public health issues. As David M. Morens says, it reflects his very wide experience in national as well as international epidemiology including:
- Pontiac fever/Legionnaires’ disease (1968/1976) [Ligeonella pneumophila – Philadelphia] First, it was thought to be a 1918-like influenza pandemic, but Mike kept running through the history of Influenza & other respiratory diseases, the epidemic ones. After a couple of days of collecting info, Mike was the first to say: “This is beginning to look like Pontiac fever.”
- Swine flu (1975–1976) [Hsw1N1 – New Jersey]
- Guillain-Barré syndrome (1977)
- Ebola hemorrhagic fever (1976) [(-)ssRNA virus – Zaire & Sudan]
- In the June 5, 1981 issue, he published a report about 5 Pneumocystis carinii pneumonia cases. Such disease was rare, so he wrote a note saying: “the case histories suggested a cellular-immune dysfunction related to a common exposure, a disease acquired through sexual contact”, which we know now as HIV/ AIDS. It was the first report about it.
- He helped in putting on the epidemiology map of Reye syndrome (1973–1977) [A fatal disease associated with Aspirin consumption when having a viral-disease e.g. Varicella – Ohio] , Kawasaki disease (1977), and toxic-shock syndrome (1980) [S. aureus]. He was consulted in the SARS outbreak in 2003 [Severe acute respiratory syndrome (+)ssRNA coronavirus] even after his full retirement.
Mike used to give the epidemiology course each July. The first subject was: “How to investigate an epidemic”. His first words were: “First, you need to find a good map…” He was teaching his students to keep an open and interested mind, to remain flexible and creative, to rethink and to assemble the puzzle pieces quickly to get the big picture.
“It’s better to be approximately right today than exactly right tomorrow,” a phrase said by Michael O’Leary, a former epidemiology student of Mike rephrasing his description of epidemiologists’ work: “Quick and dirty”.
Image credits:
Michael B. Gregg: http://www.cdc.gov/
Tags: ebola hemorrhagic fever, field epidemiology, Guillain-Barré syndrome, Michael B. Gregg, MMWR, Pneumocystis carinii, pontiac fever, reye syndrome, SARS outbreak, swine flu, toxic-shock syndrome
2 Comments »
|




 Entries (RSS)
Entries (RSS)